

Glaucoma
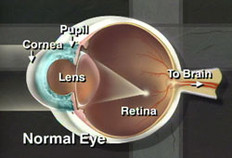
Glaucoma is a disease of the optic nerve, which carries the images we see from the eye to the brain. Glaucoma results when there is slow damage to the optic nerve due to increased pressure in the eye. This pressure is usually caused by poor drainage of the aqueous fluid out of the eye.
The most common form of glaucoma is called “primary open-angle glaucoma.” This condition is painless and the patient can slowly lose vision and not be aware of the problem until it is very advanced.
Glaucoma is a leading cause of blindness in the United States, especially for older people. If untreated, glaucoma can lead to total loss of vision, which is why early detection through routine eye exams and treatment are so important.
During your glaucoma examination, Dr. Chu or Dr. Yin will:
- Measure intraocular pressure (tonometry)
- Inspect the drainage angle of the eye (gonioscopy)
- Evaluate any optic nerve damage (ophthalmoscopy)
- Test the peripheral vision of each eye (visual field testing, or perimetry)
- Take color stereoscopic photographs of the optic nerves which are used to follow the appearance of the optic nerve
- Measure the thickness of the central cornea (pachymetry); abnormally thick or thin corneas can skew the true eye pressure measurement
Additional Testing
At Washington Eye Consultants, we are proud to have the latest state-of-the-art technologies to help diagnose and manage glaucoma, including:
- Humphrey Field Analyzer (HFA). This is a sensitive test to determine if any glaucoma damage is present. It tests the health of the specific retinal cells that can be damaged in very early glaucoma.
- OCT (Optical Coherence Tomography). This remarkable device uses ordinary light to create a CAT-scan-like cross-section of the optic nerve and nerve fiber layers to detect damage from glaucoma.
TREATMENT OF GLAUCOMA
In general, damage caused by glaucoma cannot be reversed once it has occurred. However, prompt and early treatment can help slow or prevent further damage. There are generally 3 types of treatment for glaucoma: Medication, Laser surgery (SLT), and Conventional surgery.
GLAUCOMA MEDICATIONS AND THEIR SIDE EFFECTS
Glaucoma may be controlled with eye drops taken several times a day, sometimes in combination with pills. These medications decrease eye pressure, either by slowing the production of aqueous fluid within the eye or by improving the flow leaving the drainage angle. For these medications to work, you must take them regularly and continuously. It is also important to tell all of your doctors about the eye medications you are using because glaucoma medications can have side effects and may interact with other medications you may be taking. You should notify Dr. Chu or Dr. Yin immediately if you think you may be experiencing side effects. Some eye drops may cause a stinging sensation, red eyes, blurred vision, headaches, and changes in pulse, heartbeat or breathing.
LASER SURGERY
SLT(Selective Laser Trabeculoplasty) is used to improve the drainage of the aqueous fluid out of the eye and thereby reduce the eye pressure. SLT is used to treat most types of open angle glaucoma.
Laser Peripheral Iridotomy (LPI) is used to treat most forms of narrow or closed angle glaucoma. This type of laser treatment is also performed in our office.
CONVENTIONAL SURGERY FOR GLAUCOMA
In rare cases, conventional surgery (trabeculectomy) is the only effective way of reducing eye pressure. During this procedure, a new drainage channel is created for the aqueous fluid to leave the eye.

Dry Eye Treatment
What is Dysfunctional Tear Syndrome (DTS)?
DTS, also known as dry eye syndrome, is one of the most common problems that eye doctors see. It occurs when the eyes do not produce or retain enough tears to keep its surface moist and comfortable. It is a very common, often annoying condition that, if not treated, can be serious.
What are the symptoms of DTS?
The usual symptoms include burning, aching, scratchiness, stringy mucus in or around the eyes, irritation from smoke or wind, and difficulty wearing contact lenses. Symptoms tend to be worse in dry and windy conditions, after prolonged eye use from reading or computer use, as well as late in the day. Using a hair dryer may exacerbate symptoms as may air conditioned and/or heated rooms. Many patients complain of watery eyes and are surprised to learn that their problem is dryness. The dryness is irritating to the surface of the eye, which then causes the tear-producing gland to secrete a large volume of tears. This overwhelms the tear drainage system and causes excess tears to overflow from the eye.
The most likely cause of DTS is that the eye does not produce enough tears. Tear production normally decreases as we age. Although DTS can occur in both men and women at any age, women are most often affected, particularly postmenopausal women. A wide variety of medications, both prescription and over-the-counter, can reduce tear production. Diuretics, beta blockers, antihistamines (Claritin, Zyrtec, Allegra), sleeping pills (Ambien), “nerve pills” (Prozac, Zoloft, Effexor), and pain relievers can all cause symptoms of DTS. DST can be related to some medical conditions, including rheumatoid arthritis, lupus, Sjogren’s syndrome, as well as dermatologic conditions, such as rosacea and seborrhea. DTS may also be caused by excessive tear evaporation, as may happen if you do not blink frequently enough or if your eyelids do not close well, especially when you sleep.
How is DTS diagnosed?
An ophthalmologist is usually able to diagnose DTS by examining the eyes. A new test is now available which can help diagnose dry eye in the office. The TearLab device is a non-invasive test which analyzes the tears and helps quantifiy the severity of dry eye.
How is DTS treated?
Although there is no cure for DTS, there are several treatments that can relieve the discomfort associated with it:
- Artificial Tears
Eye drops called artificial tears add moisture to the eyes, but are temporary and must be used often. Some drops are thicker and more viscous than others, and the more viscous the drop, the longer the drop is retained on the eye. However, the thicker the eye drop, the more it may blur vision. Preservative free tears are more advantageous than preserved tears because many people have a sensitivity to preservatives. Artificial tears are available over the counter without a prescription. There are many different brands, and each patient can find the best one for their individual symptoms. The tears should be used several times a day, even every hour if necessary.
- Support Measures
Simply increasing fluid intake (at least 6-8 tall glasses of fluid daily) and avoiding alcohol may improve dry eye symptoms. Also, if the air is dry (winter), increasing the humidity in your living and working areas can significantly improve eye comfort.
- Nutritional Supplements
In many cases of dry eye, the tears evaporate too quickly, leaving dry areas on the eye surface. In such cases, the oily portion of the tear film is not functioning properly. Incorporating essential fatty acids in the diet or through supplements may increase the oily portion of the tears, reduce evaporation and quiet inflammation associated with dry eyes.
- Prescription Medications
If a patient has been using artificial tears with little success, he/she may want to consider Restasis, the first and only prescription therapy for DTS. Restasis is both an artificial tear to treat symptoms in the short term, combined with medicine to treat the disease in the long term. It helps patients make their own natural tears, something an artificial tear cannot do by itself. Restasis is used twice a day—one drop in each eye, approximately 12 hours apart. It is available only by prescription.
Patients that are prescribed Restasis will usually notice more comfort and moisture within 2-4 months. Restasis may sting momentarily and this is normaVl. A second medication is usually prescribed with Restasis for the first month, and the combination of the 2 medications work very well together to improve dry eye symptoms.
- Punctal Plugs
Another simple non-surgical procedure that provides long-term relief for some patients is inserting “plugs” into the punctum, the tiny eyelid openings that drain tears into the tear ducts and nose. Once occluded, more tears are available on the eye surface. Punctal plug insertion is quick, painless, and very safe. They last indefinitely, are easily removable by the doctor for rare instances of allergy or infection, and rarely become dislodged. If plugs are to be placed, we initially place dissolvable temporary plugs in one eye as a test to see if this will work. After several days, the collagen plugs will dissolve, but prior to dissolving, they should provide significant relief in dry eye symptoms. If effective, the patient returns in 2 weeks for placement of plastic punctal plugs which will not dissolve.
- Permanent Occlusion
If none of these treatments help, the punctum can be permanently closed to prevent losing what little moisture is left. This procedure usually involves heat cautery. Afterward, patients still may need to continue using eye drops.
- LipiFlow
Many commonly attribute their eye discomfort to dry eye, when a leading cause of the burning, scratching and redness is Meibomian Gland Dysfunction or MGD.MGD occurs when there is a compromise to the function and/or structure of the Meibomian glands. These glands, located in the eyelids, produce the protective oily (lipid) layer of the tear film. This oil helps protect the surface of the eye from disease and prevents the watery part of the tears from evaporating when your eyes are open. Without these oils, the eyes become more susceptible to the negative effects that dry climates, air conditioning, computer use, reading and other daily activities can have on the long-term health of our eyes.
 Treating MGD with LipiFlow®
Treating MGD with LipiFlow®
LipiFlow® is a treatment performed in your doctor’s office designed to remove blockages from the Meibomian glands, allowing them to properly function and produce the oils that make up the top protective lipid layer of the tear film. LipiFlow® is supported by more than 30 patents with studies demonstrating its safe and effective results.1 It is designed to minimize patient discomfort during a 12-minute treatment that gently massages the eyelids.
 LipiFlow® Activators are single-use sterile devices that safely and comfortably deliver a combination of heat to the inner lids and simultaneous therapeutic motion to the outer lids, removing blockages from the Meibomian glands.
LipiFlow® Activators are single-use sterile devices that safely and comfortably deliver a combination of heat to the inner lids and simultaneous therapeutic motion to the outer lids, removing blockages from the Meibomian glands.
The Activators are contoured to avoid contact with the cornea, protecting the delicate structures of the eye.
Once the gland blockages are removed, the glands can resume normal oil or lipid production.
This oil is essential for a healthy tear film, providing stable vision and ocular comfort.
As normal gland function recovers, maximum results are usually experienced 6-8 weeks after treatment.
LipiFlow® treatment
For more information, please visit https://dryeyeandmgd.com/
None of these treatment options are mutually exclusive, and Dr. Chu or Dr. Yin may recommend a combination of these treatments, depending on the severity and the unique circumstances of each patient.
Take the Dry Eye Quiz and see if you may have Dry Eye.

Corneal Diseases
DIAGNOSIS AND TREATMENT
The cornea is the clear transparent dome in the front of the eye. In addition to allowing light to pass through the eye, the cornea does most of the bending (refracting) of light so that it can focus clearly on the retina. Corneal edema (swelling), corneal dystrophies (inherited diseases), corneal scars, injuries, and infections can cause a normal, clear cornea to become cloudy, resulting in loss of vision in one or both eyes. Some diseases such as keratoconus distort the shape of the cornea, so that the incoming light is not clearly focused on the retina. Even though the cornea appears clear in these diseases, the patient’s vision can still be very blurry.
SYMPTOMS OF CORNEAL DISEASE
- With keratoconus, as the cornea protrudes or steepens, vision becomes increasingly blurred and contact lens wear, which is often an early treatment for the disease, becomes difficult. The contact lens may not stay on the eye due to the irregular shape of the cornea.
- A person with Fuchs’ endothelial dystrophy or bullous keratopathy may first notice glare with lights at night or in bright sunlight. As these conditions progress, vision may be foggy or blurry in the morning and clear up as the day progresses. As the diseases further progress, vision will stay blurrier later into the day and eventually may not clear at all.
- Some corneal diseases can be very painful.
Keratoconus is a weakening and thinning of the central cornea. The cornea develops a cone-shaped deformity. The condition is often diagnosed with . Progression can be rapid, gradual or intermittent. Keratoconus usually occurs in both eyes, but can occur in only one eye.
Fuchs’ endothelial dystrophy is a hereditary abnormality of the inner cell layer of the cornea called the endothelium. The purpose of this layer is to pump fluids out of the cornea, keeping it thin and crystal clear. Early on, this dystrophy is noticed only by your eye doctor using a slit-lamp microscope. When the endothelium progressively loses its function, fluids are not pumped out and the cornea can develop swelling, causing it to become cloudy and decrease vision. This condition is often diagnosed with specular microscopy.
Bullous keratopathy is a condition in which the cornea becomes permanently swollen. This condition can occur as a late stage of corneal dystrophies such as Fuchs’ endothelial dystrophy (above). Bullous keratopathy can also occur because the inner layer of the cornea, the endothelium, has been damaged and is no longer pumping fluids out of the tissue.
TYPES OF CORNEAL DISEASE
- Infection: Bacterial and viral infections are common causes of corneal damage; fungal uncommon. In third world countries, corneal infections are a common cause of blindness.
- Keratoconus: The cause of keratoconus in most patients is unknown.
- Age: Aging processes can affect the clarity and health of the cornea
- Cataract and intraocular lens implant surgery: Bullous keratopathy occurs in a very small percentage of patients following these procedures.
- Heredity (for example, corneal dystrophies)
- Contact lenses
- Eye trauma
- Certain eye diseases, such as retinitis pigmentosa, retinopathy of prematurity, and vernal keratoconjunctivitis.
- Systemic diseases, such as Leber’s congenital amaurosis, Ehlers-Danlos syndrome, Down syndrome and osteogenesis imperfecta.
DIAGNOSE CORNEAL DISEASE
Your eye doctor can check for corneal disease and trauma by examining your eyes with magnifying instruments, the most important of which is a slit lamp. Other such as corneal topography can help your doctor detect early cataracts, corneal scars, and other problems associated with the front structures of the eye. After dilating your eyes, your doctor will also examine your retina for early signs of disease.
TREATMENT CORNEAL DISEASE
Some corneal diseases are easily treatable with new glasses or simply with drops. Many cases of keratoconus can be treated with special contact lenses. More severe corneal scars, advanced dystrophies, and advanced keratoconus are often treated with corneal transplant surgery.

Retinal Diseases
The retina is a very thin, but complex tissue that lines the back of the eye. It is composed of millions of cells, including photoreceptor cells that sense light and send images to the brain.
There are many conditions that can impair the retina’s ability to receive and transmit images. The most common retinal diseases are diabetic retinopathy, age-related macular degeneration, and retinal detachments. These conditions are all very serious and if not treated, can lead to loss of vision.
EXAMINATION OF THE RETINA
A retinal examination is the only way to properly diagnose retinal problems. Serious retinal diseases can often be treated before the patient begins to experience vision problems. During the exam the ophthalmologist first dilates the pupil using drops and then looks inside the eye with an ophthalmoscope, a device that allows the physician to clearly see the retina.
Another effective test is the Optical Coherence Tomography (OCT), a new technology we are pleased to offer at The Rhode Island Eye Institute. This rapid imaging device bounces light rays off the retina and the reflections are transmitted to a computer. The result is a detailed 3-D cross-section of the retina.
TREATMENT OF RETINAL DISEASES
Many retinal diseases can be treated with various forms of laser light. These very powerful light beams can help destroy abnormal blood vessels in the retina or act to seal off retinal tears. Laser therapy is usually done in our office with anesthetic drops or anesthetic injection around the eye to ease any discomfort.
Other retinal diseases require surgery. Most retinal surgery involves first removing the vitreous gel (the clear fluid inside the eye), and then using delicate instruments to remove any abnormal tissue from the surface of the retina. Retinal surgery is usually done in a hospital operating room with a local anesthetic.
DIABETIC RETINOPATHY TREATMENT
Diabetic retinopathy results when blood vessels in the retina are damaged due to high blood-sugar levels in people with diabetes.
Prevention through strict control of blood sugar levels is the best way to reduce the long-term risk of vision loss from diabetic retinopathy. For more advanced diabetic retinopathy, laser treatment is often recommended. Sometimes retinal surgery is required.
AGE-RELATED MACULAR DEGENERATION
Age-related macular degeneration (AMD) is the leading cause of legal blindness in the United States. In fact, 2.2% of people 65 years or older have severe vision problems from the disease.
AMD is a disease that affects the macula, the small area in the center of the retina that allows fine details to be seen clearly. Despite the fact that the macula takes up only 3% of the retinal surface area, it is responsible for all detailed vision, such as reading, artwork, seeing the face of a clock, etc. An eye affected by macular degeneration will not be able to perceive details or colors as well as a healthy eye.
The first sign of macular degeneration may be the need for more light when you do close –up work. Fine print may become harder to read and street signs more difficult to recognize. The condition usually develops gradually, but may sometimes progress more quickly, leading to severe vision loss in one or both eyes.
The condition tends to develop as you get older, hence the term, “age-related. Macular degeneration is the leading cause of severe vision loss in people age 60 or older.
There are two forms of macular degeneration: “dry” macular degeneration and “wet” macular degeneration. The dry form is more common and is caused by aging and thinning of the cells in the macula. Vision loss is slow and gradual.
The “wet” form occurs in only 10% of patients with AMD and causes much more rapid, and usually more serious, loss of vision. This loss of vision is due to the growth of abnormal fragile blood vessels in or near the macula. These blood vessels leak blood or fluid and blur central vision quickly. Untreated wet AMD can lead to scarring of the macular area and permanent vision loss.
TREATMENT OF AGE-RELATED MACULAR DEGENERATION
There is no cure for dry AMD, though various combinations of vitamins and anti-oxidant pills have been shown to help slow down the progress of the disease.
Some treatment options are available for wet macular degeneration, including Photocoaguation (Argon Laser Therapy, Photodynamic Therapy (PDT), Visudyne®, Macugen®, Avasin and Transpupillary Thermotherapy (TTT).
Photocoagulation: Argon Laser Therapy
In photocoagulation, the doctor uses a high-energy laser beam to create small burns in areas with abnormal blood vessels. It can prevent further damage to the macula and halt continued vision loss.
Photodynamic therapy (PDT)
This therapy is for treatment CNV or abnormal blood vessels that is located directly under the fovea. The fovea lies at the center of your macular and in healthy eyes provides your sharpest vision. PDT increases your chances of preserving some of that vision. It won’t bring back vision you have lost, but it may halt the loss of your vision or at least slow down the rate of vision
loss.
Transpupillary Thermotherapy
TTT are a technique that uses a state-of-the-art diode laser to slowly deliver heat through the pupil to the abnormal blood vessels in the retina. The heat from the laser destroys the abnormal vessels to stop or slow the effects of macular degeneration.
EMERGING TREATMENTS
Macugen
Approved by the Food and Drug Administration in December 2004, pegaptanib, (Macugen) is a drug used for treatment of wet macular degeneration. The drug stops the formation of new blood vessels and decreases leakage from existing blood vessels. Macugen, given as a series of injections into the vitreous fluid in the eye, may prevent further loss of vision.
Lucentis
Like Macugen, ranibizumab (Lucentis) is another drug to treat wet macular degeneration by impeding new growth of abnormal blood vessels. Lucentis shows promise in reversing the effects of macular degeneration, not just preventing further vision loss. Lucentis is currently available only in clinical trials; however, it is being prescribed using a closely related drug, bevacizumab (Avastin).
Visudyne®
Visudyne is a light-activated drug that is injected into the blood stream and travels to the abnormal blood vessels in the macula where it collects. A “cold” PDT laser activates the medication and closes the abnormal blood vessels without causing damage to the healthy retina. The therapy may be reapplied at three-month intervals as needed.
Transpupillary Thermotherapy (TTT )
Transpupillary Thermotherapy (TTT) is a technique that uses a state-of-the-art diode laser to slowly deliver heat through the pupil to the abnormal blood vessels in the retina. The heat from the laser destroys the abnormal vessels to stop or slow the effects of macular degeneration.
RETINAL DETACHMENT
Almost all retinal detachments start with a small tear in the retina, which allows fluid to go behind the retina and push it out of its normal position in the back of the eye. Detachments are very serious and almost always lead to blindness if not treated promptly.
TREATMENT OF RETINAL DETACHMENT
Most retinal tears (the early stage of retinal detachment) are treated with laser surgery or cryotherapy (freezing), both of which reattach the retina to the back wall of the eye. This treatment usually prevents retinal detachment and is performed in the doctor’s office with little to no discomfort.
A retinal detachment requires surgery to first seal the tear and then reattach the retina back in its proper position. There are several types of surgery used, and the decision of which type depends upon the characteristics of the detachment. Some retinal detachments can be treated in the doctor’s office, using an injection of air inside the eye to push the retina back into position. However, most detachments require surgery in a hospital operation room.

Pterygium and Pingueculum
WHAT IS A PTERYGIUM?
A pterygium is a fleshy growth that invades the cornea (the clear front dome of the eye).
It is an abnormal process in which the conjunctiva (a membrane which covers the white of the eye) grows into the cornea. A pterygium may be small or grow large enough to interfere with vision and commonly occurs on the inner comer of the eye.
WHAT CAUSES A PTERYGIUM?
A pterygium occurs more often in people who spend a great deal of time outdoors, especially in sunny climates. Long-term exposure to sunlight, especially ultraviolet (UV) rays is the main cause.
HOW IS A PTERYGIUM TREATED?
We specialize in the surgical removal of pterygium., but sometimes, when a pterygium becomes red and irritated, topical eyedrops or ointments may be used initially to reduce the inflammation. The indications for surgical removal of a pterygium are: 1) prolonged discomfort and redness not relieved by eye drops 2) growth onto the cornea causing poor vision or inability to wear contact lenses, and 3) cosmetically objectionable. Surgical treatment is a very successful and effective method of treating pterygia. However, there is a chance that the pterygium may return. Protecting the eyes from UV light with proper sunglasses may help to prevent recurrences.
WHAT IS A PINGUECULUM?
A pingueculum is a yellowish or pink patch or bump on the white of the eye. It is not a tumor, but an alteration of normal tissue resulting in a deposit of abnormal protein and fat. Unlike a pterygium, a pingueculum does not actually grow onto the cornea. A pingueculum may grow to become a pterygium, and also develops in response to chronic eye irritation and sunlight.
HOW IS A PINGUECULUM TREATED?
No treatment is necessary unless it becomes inflamed. A pingueculum does not threaten sight, but may progress to a pterygium unless the eye is protected from irritation and sunlight. If particularly annoying, a pingueculum may be surgically removed.
WHY ARE REGULAR MEDICAL EYE EXAMS IMPORTANT FOR EVERYONE?
Eye disease can occur at any age. Many eye diseases do not cause symptoms until the disease has done damage. Since most blindness is preventable if diagnosed and treated early, regular medical exams by an ophthalmologist are very important. Why an ophthalmologist? Because an ophthalmologist provides total eye care: medical, surgical, and optical.